
A couple of years ago, the British medical journal The Lancet asked a group of experts to assess the global state of surgery. The panel now reports finding a major gap between the need for surgery and what is actually available, especially in low- and middle-income countries.
In its report published by The Lancet, the group says people are dying from conditions easily treated in the operating room such as hernia, appendicitis, obstructed labor, and serious fractures.
Stanford University surgery professor Thomas Weiser, a member of The Lancet commission, says the need is great.
“There are probably about 143 million [additional] operations [a year] that are needed just to meet basic needs in low- and middle-income countries," said Weiser. "There are probably about five billion people that don’t have access to safe, timely surgery with protection against catastrophic expenditure. And so, those are pretty big numbers.”
The Lancet commission notes “remarkable gains” in global health over the last quarter-century, but says surgery has not kept up with advances in other areas.
“You can’t achieve universal health care if you don’t incorporate surgery," said Harvard Medical School’s John Meara who is one of the lead authors of The Lancet paper.

Meara said increasing the availability of surgical treatments is not as simple as providing bedding nets designed to protect against malaria. Surgery requires trained staff, proper facilities and sterile instruments, but also reliable electricity, a system for getting patients to often-distant hospitals, and a business model that does not bankrupt those who need an operation.
The report suggests spending an additional $300 to $420 billion on surgery between now and 2030. That's a lot of money, but Meara says The Lancet commission calculated each dollar spent would return three or four dollars in economic benefit from lives saved and people returned to productive good health.
“When you look at cost effectiveness in terms of dollars spent, for welfare gains, for the positive impact on human beings, surgery is every bit as cost-effective as any of those other aspects,” Meara said.
There is no one best path to improving access to surgery, and the report cites several diverse countries, including Mexico and Rwanda, as having taken steps toward improving access to surgical services.
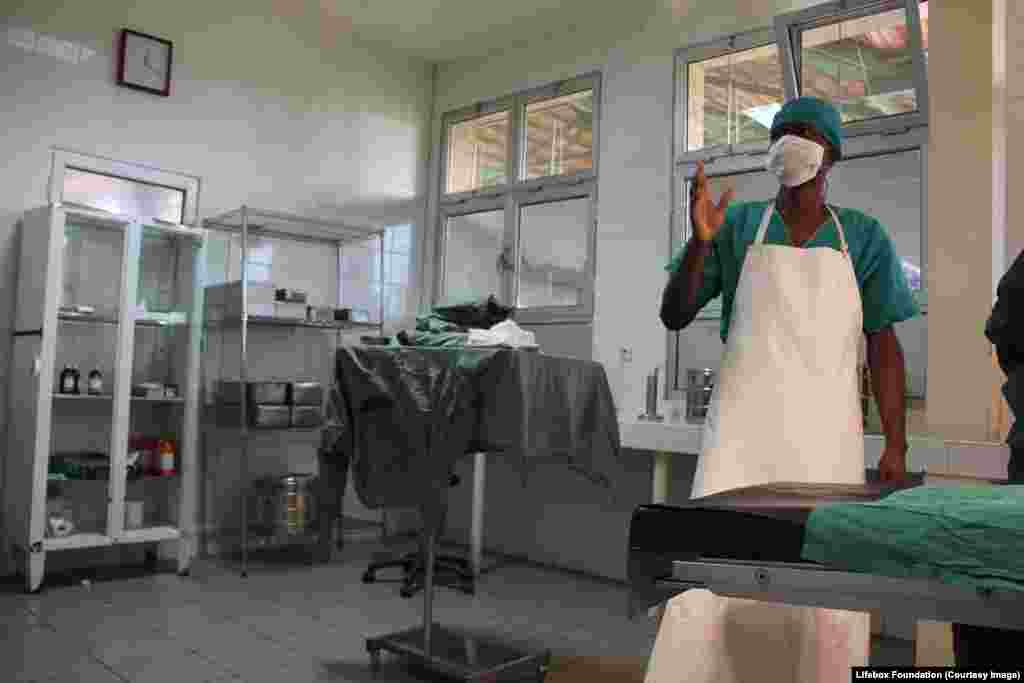
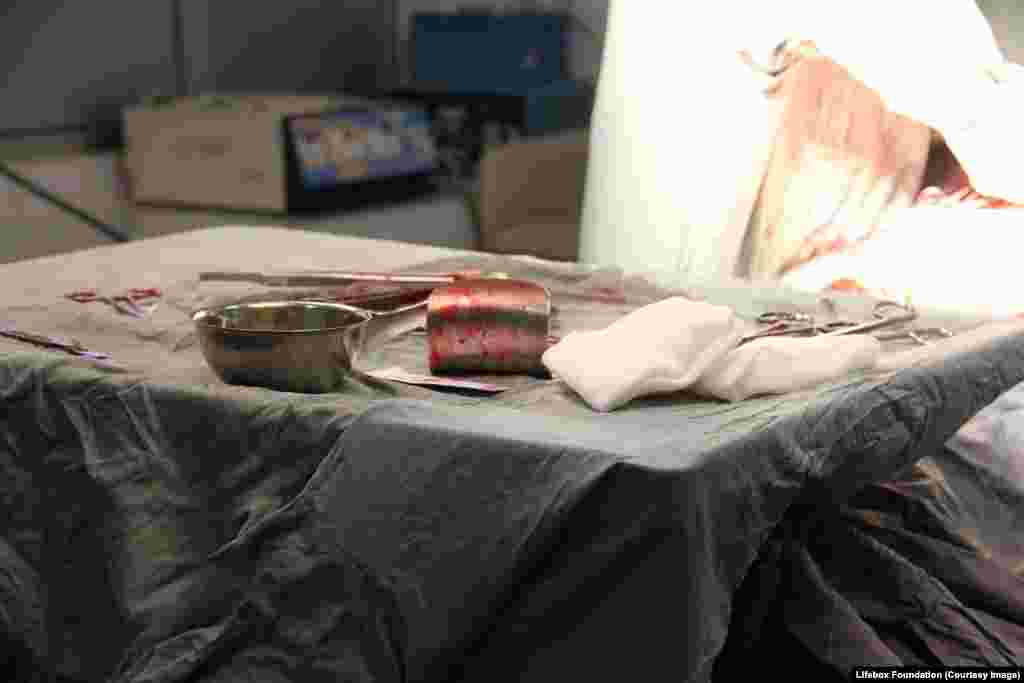
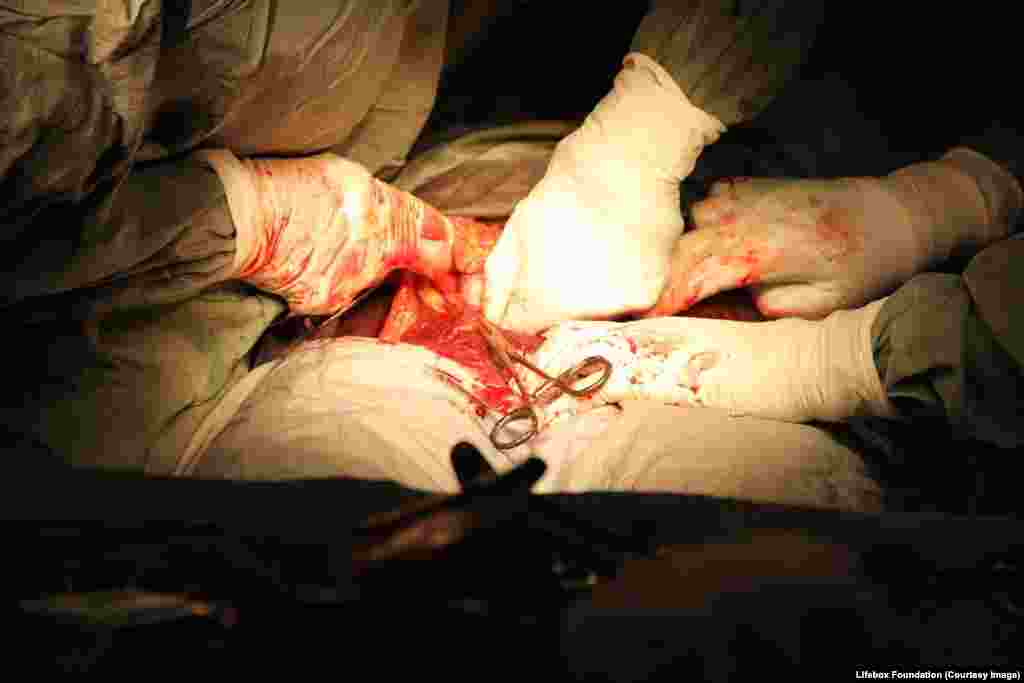
Surgery in Low Resource Settings





![Female patient monitored using Lifebox pulse oximeter [essential oxygen monitor] during emergency Caesarean section.](https://gdb.voanews.com/4696ccbb-aac9-40bf-bf45-16af6d9b7dc0_w1024_q10_s.jpg)








![Young girl on the ward at a hospital, leg in traction, recovering from osteotomy [bone cut] to correct bow legs.](https://gdb.voanews.com/f68650fb-95ac-4bdf-9d9c-0f4fbcfea0f2_w1024_q10_s.jpg)